Chêneau Bracing
Weiss HR, Moramarco M (2020) Orthotics: Schroth’s Textbook of Scoliosis and Other Spinal Deformities. Edited by Moramarco, M, Borysov M, Ng SY, Weiss HR. 656-696 Newcastle upon Tyne: Cambridge Scholars Publishing. ISBN: 978-1527538290.
Cinella et al. The treatment of adolescent idiopathic scoliosis with Cheneau brace: long term outcome. Scoliosis. 2009; 4(Suppl 2): O44.
Conclusions: At the end of treatment we observed an improvement in correction around at 23% (p value < 0.05) from the beginning curves, and after 5 years there was stabilization at approximately15% (p value < 0.05). Our results demonstrate that conservative treatment with the Cheneau brace is corrective for the treatment of I.S.
Cheneau-Gensingen® Brace by Weiss (GBW)
Weiss HR, Turnbull D, Seibel S, Kleban A. First end-result of a prospective cohort with AIS treated with a CAD Chêneau style brace. J Phys Ther Sci. 2019;31(12):983–991.
Conclusions: The results achieved in this study, which included a cohort of patients braced in the Cheneau Gensingen brace (GBW), are comparable and significantly better than the results achieved with the Boston Brace. The Cheneau Gensingen Brace resulted in a 92.9% success rate for the braced cohort.
Weiss HR, Tournavitis N, Seibel S, Kleban A. A Prospective Cohort Study of AIS Patients with 40° and More Treated with a Gensingen Brace (GBW): Preliminary Results The Open Orthopaedics Journal 2017;11 (Suppl-9, M8): 1558-1567.
Conclusions: Conservative brace treatment using the Gensingen brace was successful in 92% of cases of patients with AIS of 40 degrees and higher. This is a significant improvement compared to the results attained in the BrAIST study (72%). Reduction of the ATR shows that postural improvement is also possible.
Weiss HR, Seibel S, Moramarco M, Kleban A. Bracing Scoliosis – the Evolution to CAD/CAM Hard Tissue 2013 November. 2: 5.43.
Conclusions: Symmetrical braces for scoliosis are outdated. Asymmetric braces allow better in-brace correction compared to symmetric braces.
Weiss HR. “Brace technology” thematic series – the Gensingen brace™ in the treatment of scoliosis. Scoliosis. 2010 Oct 13;5:22.
Conclusion: The use of the Gensingen brace® leads to sufficient in-brace corrections, when compared to the correction effects achieved with other braces, as described in literature. According to the patients’ reports, the Gensingen brace® is comfortable to wear, when adjusted properly.
Weiss HR, Werkmann M. Rate of surgery in a sample of patients fulfilling the SRS inclusion criteria treated with a Chêneau brace of actual standard. Stud Health Technol Inform. 2012;176:407–410.
Conclusion: Surgery incidence can be reduced with Chêneau (Gensingen) brace when satisfactory in-brace correction occurs. Clinical outcomes make a difference for when it comes to patient satisfaction.
Weiss HR, Moramarco M. Remodeling of trunk and backshape deformities in patients with scoliosis using standardized asymmetric CAD / CAM braces. 2013 Feb. Hard Tissue 26;2(2): 2.14.
Conclusion: Trunk and backshape can be improved conservatively even with curvatures exceeding 45º and maybe even improve scoliotic deformities radiographically.
Scoliosis Bracing information: impromptu interview with Dr. Weiss – May 2013, Germany
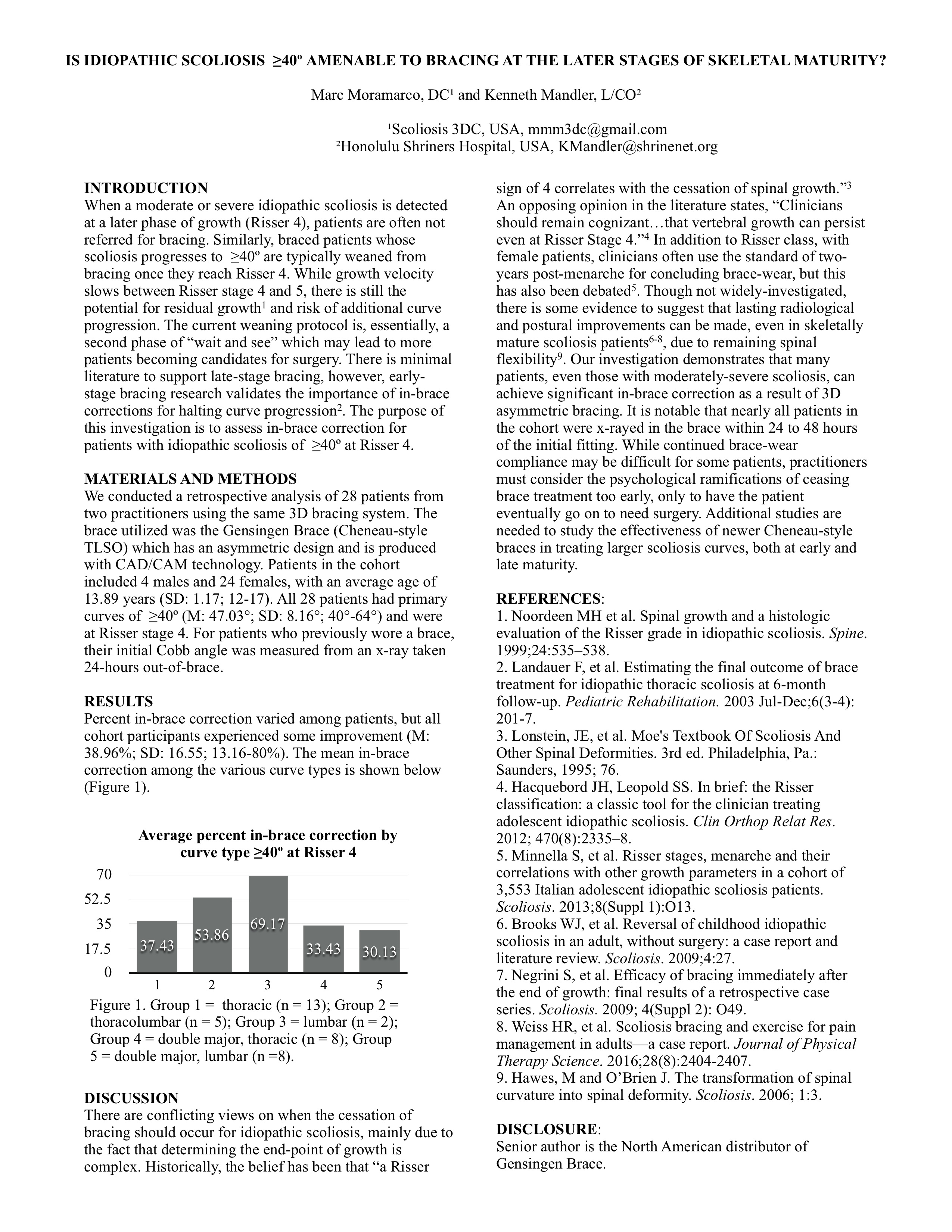
Presentation: AOPA, National Assembly, September 2017, Las Vegas, NV Marc Moramarco, DC and Ken Mandler, L/CO: Is Idiopathic Scoliosis ≥ 40º Amenable to Bracing at the Later Stages of Skeletal Maturity?
{kind=link}
Scoliosis Bracing
Weinstein SL, Dolan LA, Wright JG, Dobbs MB. Effects of Bracing in Adolescents with Idiopathic Scoliosis N Engl J Med. 2013 Oct 17;369(16):1512-21.
Conclusions: “Bracing significantly decreased the progression of high-risk curves to the threshold for surgery in patients with adolescent idiopathic scoliosis. The benefit increased with longer hours of brace wear.”
Wong et al. The effect of rigid versus flexible spinal orthosis on the clinical efficacy and acceptance of the patients with adolescent idiopathic scoliosis. Spine. 2008 May 20;33(12):
Conclusion: The current study showed that the failure rate of the SpineCor was significantly higher than that of the rigid spinal orthosis, and the patients’ acceptance to the SpineCor was comparable to the conventional rigid spinal orthosis.
Nachemson AL, Peterson LE. Effectiveness of treatment with a brace in girls who have adolescent idiopathic scoliosis. A prospective, controlled study based on data from the Brace Study of the Scoliosis Research Society. J Bone Joint Surg Am. 1995 Jun;77(6):815-22.
Conclusion: Effectiveness of treatment with a brace in girl who have adolescent idiopathic scoliosis. A prospective, controlled study based on data from the brace study of the scoliosis research society.
Lange et al. Long-term results after Boston brace treatment in late-onset juvenile and adolescent idiopathic scoliosis. Scoliosis 2011, 6:18
Conclusions: Long-term results were satisfactory in most of 272 patients with late-onset juvenile and AIS treated with Boston brace in average 24.7 years earlier. Nine percent had surgery and 13% had curve progression to ≥ 45° at follow-up. HRQL was slightly decreased in these patients, SRS-22 scores for self-image was significantly lower in both groups. Self-report indicates that future patients can be reassured that scoliosis does not affect pregnancy and delivery, and that most patients are expected to work and have HRQL in the normal range at long-term.
Fayssoux RS, Cho RH, Herman MJ. A History of Bracing for Idiopathic Scoliosis in North America. Clinical Orthopaedics and Related Research. 2010;468(3):654-664.
Conclusions: The goals of brace treatment for AIS are to prevent progression of deformity and to obviate the need for spinal fusion, not to improve the deformity.
Castro FP Jr. Adolescent idiopathic scoliosis, bracing, and the Hueter-Volkmann principle. Spine J. 2003 May-June; 3(3):180.5.
Conclusion: Brace application results in immediate positional derotations of the spine in patients with AIS. These positional derotations were maintained only in patients with flexible curves, at final follow-up. Brace treatment was not recommended in patients whose curves did not correct at least 20% in a TLSO.
Scoliosis Exercise
Moramarco M, Moramarco K, Fadzan M. Cobb Angle Reduction in a Nearly Skeletally Mature Adolescent (Risser 4) After Pattern-Specific Scoliosis Rehabilitation (PSSR). The Open Orthopaedics Journal 2017;11(Suppl-9, M4):1490-1499.
Monticone M, Ambosini E, Cazzaniga D, Rocca B. Active self-correction and task-oriented exercises reduce spinal deformity and improve quality of life in subjects with mild adolescent idiopathic scoliosis. Results of a randomized controlled trial. Eur Spine J. 2014 Feb 28.
Weiss HR, Seibel S. Scoliosis short-term rehabilitation (SSTR) —a pilot investigation. The Internet Journal of Rehabilitation. 2010
Weiss HR, Hollaender M, Klein R. ADL based scoliosis rehabilitation—the key to an improvement of time-efficiency? Stud Health Technol Inform. 2006;123:594–598.
Weiss HR, Klein R. Improving excellence in scoliosis rehabilitation: a controlled study of matched pairs. Pediatr Rehabil. 2006;9:3. 190–200 Jul/Sep.
Weiss HR, Lehnert-Schroth C, Moramarco M. Schroth Therapy – Advancements in Conservative Scoliosis Treatment. Lambert Academic Publishing, Saarbruecken 2015.
Weiss HR. The effect of an exercise program on VC and rib mobility in patients with IS. Spine. 1991;16:88–93.
Borysov M, Borysov A. Scoliosis short-term rehabilitation (SSTR) according to ‘Best Practice’ standards – are the results repeatable? Scoliosis. 2012 Jan 17;7(1):1.7.
Pugacheva, N. Corrective exercises in multimodality therapy of idiopathic scoliosis in children – analysis of six weeks efficiency – pilot study. Stud Health Technol Inform. 2012; 176:365-371.
Lee SG. Improvement of curvature and deformity in a sample of patients with Idiopathic Scoliosis with specific exercises. OA Musculoskeletal Medicine. 2014; Mar 12;2(1):6.
Maruyama T, Matsushita T, Takeshita K, Kitagawa K, Nakamura K, Kurokawa T: Side shift exercises for idiopathic scoliosis after skeletal maturity. Journal of Bone and Joint Surgery (Br) 2003; 85B; Supp 1: 89.
Fusco C, Zaina F, Atanasio S, Romano M, Negrini A, Negrini S: Physical exercises in the treatment of adolescent idiopathic scoliosis: an updated systematic review. Physiother Theory Pract. 2011; Jan;27(1):80-114.
Weiss HR, Weiss G, Petermann F. Incidence of curvature progression in idiopathic scoliosis patients treated with scoliosis inpatient rehabilitation (SIR): an age- and sex-matched controlled study. Pediatr Rehabil. 2003;6(1):23–30.
Otman S, Kose N, Yakut Y: The efficacy of Schroth s 3-dimensional exercise therapy in the treatment of adolescent idiopathic scoliosis in Turkey. Saudi Medical Journal 2005; 26: 1429–1435.
Negrini, Stephano, et al., Physical exercises as a treatment for adolescent idiopathic scoliosis, a systematic review. Pediatric Rehabilitation, 2003, Vol. 6, No. 3-4, 227-235.
Weiss, Hans-Rudolf, M.D., Influence of an in-patient exercise program on scoliotic curves., Italian Journal of Orthopaedics and Traumatology, 1992.
Weiss, Hans-Rudolf, M.D., The Progression of Idiopathic Scoliosis under the Influence of a Physiotherapy Rehabilitation Program, Physiotherapy, November, 1992.
Schreiber S, Parent EC, Moez EK, et al. The effect of Schroth exercises added to the standard of care on the quality of life and muscle endurance in adolescents with idiopathic scoliosis—an assessor and statistician blinded randomized controlled trial: “SOSORT 2015 Award Winner.” Scoliosis. 2015;10:24. doi:10.1186/s13013-015-0048-5.
Asymmetric Spinal Loading
Scoliosis Etiology Theories
Fadzan M, Bettany-Saltikov J. Etiological Theories of Adolescent Idiopathic Scoliosis: Past and Present. The Open Orthopedics Journal 2017;11(Suppl-9, M3): 1466-1489.
Burwell, R.G.: Aetiology of idiopathic scoliosis: current concepts Pediatric Rehabilitation, 2003, Vol. 6, No. 3-4, 137-170.
Chu WC, Lam WM, Ng BK, et al. Relative shortening and functional tethering of spinal cord in adolescent scoliosis – Result of asynchronous neuro-osseous growth, summary of an electronic focus group debate of the IBSE. Scoliosis. 2008;3:8. doi:10.1186/1748-7161-3-8.
Girardo M, Bettini N, Dema E, Cervellati S. The role of melatonin in the pathogenesis of adolescent idiopathic scoliosis (AIS). European Spine Journal. 2011;20(Suppl 1):68-74. doi:10.1007/s00586-011-1750-5.
Scoliosis and Long-Term Effects
Asher A, Burton D. Adolescent idiopathic scoliosis: natural history and long term treatment effects. Scoliosis 2006, 1:2 doi:10.1186/1748-7161-1-2
Danielsson A. Natural history of adolescent idiopathic scoliosis: a tool for guidance in decision of surgery of curves above 50°. Journal of Children’s Orthopaedics. 2013.
Weinstein S. Health and Function of Patients With Untreated Idiopathic Scoliosis – A 50-Year Natural History Study. JAMA, 2003;289(5):559-567. doi:10.1001/jama.289.5.559
Scoliosis and Pain
Weiss HR. Scoliosis-related pain in adults – treatment influences. Eur J Phys Rehabil Med. 1993;3:91–94.
Schreiber S, Parent EC, Moez EK, et al. The effect of Schroth exercises added to the standard of care on the quality of life and muscle endurance in adolescents with idiopathic scoliosis—an assessor and statistician blinded randomized controlled trial: “SOSORT 2015 Award Winner.” Scoliosis. 2015;10:24. doi:10.1186/s13013-015-0048-5.
Upasani VV, Caltoum C, Petcharaporn M, Bastrom TP, Pawelek JB, Betz RR, et al. Adolescent idiopathic scoliosis patients report increased pain at five years compared with two years after surgical treatment. Spine. 2008;33:1107–12. doi: 10.1097/BRS.0b013e31816f2849.
Scoliosis and the Sagittal Plane
van Loon PJ, Kühbauch BA, Thunnissen FB. Forced lordosis on the thoracolumbar junction can correct coronal plane deformity in adolescents with double major curve pattern idiopathic scoliosis. Spine. 2008 Apr 1;33(7):797–801.
Conclusions: “Scoliosis deformities are significantly reduced in supine position by a lordotic fulcrum force on the thoracolumbar junction. These findings may have consequence on bracing techniques.
Schlösser TP et al. Differences in early sagittal plane alignment between thoracic and lumbar adolescent idiopathic scoliosis. Spine J. 2014 Feb 1;14(2):282-90.
Conclusion: This study demonstrates that even at an early stage in the condition, the sagittal profile of thoracic adolescent idiopathic scoliosis differs significantly from lumbar scoliosis, and both types of scoliosis differ from controls, but in different aspects. This supports the theory that differences in underlying sagittal profile play a role in the development of different types of idiopathic scoliosis.
Weiss HR, Dallmayer R, Gallo R. Sagittal counter forces (SCF) in the treatment of idiopathic scoliosis: a preliminary report. Pediatr Rehabil 9:1; 2006:24-30 Jan/Mar.
Conclusion: The application of sagittal counter forces (SCF) seems to have similar short-term effects as 3D correction and should be addressed more in future concepts of scoliosis bracing.
Scoliosis Screening
Timothy A Mirtz*, Mark A Thompson, Leon Greene, Lawrence A Wyatt and Cynthia G Akagi. Adolescent idiopathic scoliosis screening for school, community, and clinical health promotion practice utilizing the PRECEDE-PROCEED model. Chiropr Osteopat. 2005; 13: 25.
Weiss, Hans-Rudolf, M.D., et al., Indications for conservative management of scoliosis(guidelines), SOSORT, v1:5, 2006.
Scoliosis and Self-Esteem
Weiss HR, Cherdron J. Effects of Schroth’s rehabilitation program on the self concept of scoliosis patients Rehabilitation. 1994; 33:1. 31-34 Feb.
Scoliosis Surgery
Westrick ER, Ward WT. Adolescent idiopathic scoliosis: 5 year to 20-year evidence-based surgical results. J Pediatr Orthop. 2011;31(1 Suppl):S61–S68.
Weiss HR, Moramarco M, Moramarco K. Risks and long-term complications of adolescent idiopathic scoliosis surgery vs. non-surgical and natural history outcomes. Hard Tissue. 2013;2(3):27.
Weiss HR, Goodall D. Rate of complications in scoliosis surgery – a systematic review of the Pub Med literature. Scoliosis. 2008;3:9. doi: 10.1186/1748-7161-3-9.
Mueller FJ, Gluch H. Cotrel-dubousset instrumentation for the correction of adolescent idiopathic scoliosis. Long-term results with an unexpected high revision rate. Scoliosis. 2012;7(1):13. doi: 10.1186/1748-7161-7-13.
Hawes MC, O’Brien JP. A century of spine surgery: what can patients expect? Disabil Rehabil. 2008;30(10):808–17. doi: 10.1080/09638280801889972.
Hawes M. Impact of spine surgery on signs and symptoms of spinal deformity. Pediatr Rehabil. 2006;9(4):318–39. doi: 10.1080/13638490500402264.
Scoliosis and Sports
Zaina, Fabio et al. Swimming and Spinal Deformities: A Cross-Sectional Study. The Journal of Pediatrics , Volume 166 , Issue 1 , 163 – 167.
Tanchev PI, Dzherov AD, Parushev AD, Dikov DM, Todorov MB. Scoliosis in rhythmic gymnasts. Spine. 2000;25(11):1367–1372.
Longworth B, Fary R, Hopper D. Prevalence and predictors of adolescent idiopathic scoliosis in adolescent ballet dancers. Arch. Phys. Med. Rehabil. 2014;95:1725–30.
The National Scoliosis Foundation for information and scoliosis forums:
Please take the NSF forum with a grain of salt. You may surely run across some useful information, but if you are new to the forum, you will soon discover that most threads are one-sided in favor of surgery and the forum is dominated by the same posters day in and day out, many for the twelve years we have been involved in the field. Many of the surgery focused posters will post on the non-surgical threads and have a closed mind about any complementary approach. A healthy skepticism is wise, however most posters have already had surgery or their children have surgery, so their viewpoints are understandable.