Scoliosis and x-rays go hand and hand but parents, and even some kids, have concerns about x-ray frequency to monitor spinal changes during growth. We understand the concerns about scoliosis and x-rays and figured it is about time to address them.
X-ray evaluation is a necessary part of monitoring scoliosis. X-rays allow physicians to measure Cobb angles, identify spinal and rib deformations, and monitor curvature changes. Though radiation exposure is a legitimate concern, according to the Health Physics Society, “There is no conclusive evidence of radiation causing harm at the levels patients receive from diagnostic x-ray exams” (1). A study, specific to scoliosis radiology states, “Patients undergoing scoliosis radiography receive effective doses that are low in comparison with other types of radiographic examination” (2).
During adolescence, scoliosis monitoring can be frequent to monitor changes/progression that can occur in a very short span of time during a growth spurt. While no one wants unnecessary X-rays, treatment based on a dated X-ray is not in an adolescent’s best interest. For adults, scoliosis and X-rays are not as much of an issue since there is usually no need to monitor scoliosis as frequently as adolescent patients who are actively growing. However, for the purposes of embarking on a new scoliosis treatment program, for an adult, a three or four-year-old image is too old, especially when pain is present.
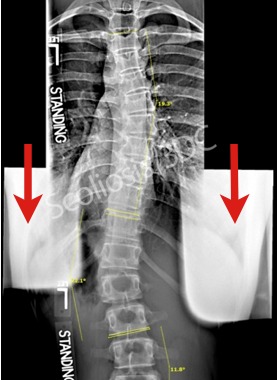
When it comes to the Schroth Method and Chêneau scoliosis bracing programs here at Scoliosis 3DC®, x-rays help us to properly identify curve pattern (accurate management decisions depend on it). A current x-ray allows us to obtain accurate baseline Cobb angle measurements. We usually only require two views of the full spine, known as a ‘scoliosis series.’ One x-ray view is of the full spine – an AP (anterior to posterior) or PA (posterior to anterior) view. The other is a sagittal (side-view) of the spine. After the initial evaluation, we request just one follow-up (the AP or PA) view for check-ups for growing kids. Frequency depends upon each case – depending on curve severity and bone maturity (Risser sign).
When having x-rays, patients should take precautions to minimize radiation effects. Experts recommend standing at least six feet away from the x-ray unit to decrease the amount of radiation received (the farther from the x-ray unit, the less radiation exposure). Since soft tissue is more susceptible to radiation effects compared to bone, we recommend the PA view vs the AP view. The ovaries/genital area can be shielded but you will probably need to request this. This should be standard procedure but it doesn’t appear to be based on the x-rays we see. Patients/parents need to be their own best advocate when it comes to reducing scoliosis x-ray exposure. Compared to conventional radiology, newer digital x-ray equipment minimizes exposure. Therefore, it might be better to have X-rays taken at a facility with modern digital equipment when possible.
For parents and patients who are highly concerned about scoliosis and X-rays, look for an electro-optical sensor (EOS) imaging center. EOS is said to offer better image quality with significantly reduced exposure when compared to conventional x-rays (up to 10X less according to Children’s Hospital of Wisconsin – one of the first U.S. facilities to offer EOS). While EOS is expensive, if you have significant concerns about radiation exposure, you may want to locate an EOS center as an alternative to conventional X-ray facilities. Usually, EOS is found in hospitals and compared to just a few years ago the number of U.S. facilities offering EOS has increased quickly. At Scoliosis 3DC®, we refer to Boston’s Children’s Hospital for EOS x-rays.
A study entitled, “Management decisions for adolescent idiopathic scoliosis significantly affect patient radiation exposure” notes that there are significant differences in the total radiation exposure in scoliosis patients who have had different treatments (Spine 2012). Researchers from this study concluded that,
“…operative patients receiv[ed] approximately 8 to 14 times more radiation than brace patients or those undergoing observation alone, respectively. Operative patients also receive more than twice the radiation per year than braced or observed patients. Almost 78% of the annual radiation exposure for operative patients occurs intraoperatively (3).”
It should be noted that the determination about radiation exposure of operative patients was determined to be primarily due to computed tomography (CT) scans and intraoperative fluoroscopy at the time of surgery. However, it does serve to underscore yet another benefit of avoiding surgery for scoliosis and approaching scoliosis management using an effective conservative treatment program like ours.
If radiation is your concern, embarking on the proactive path (don’t wait and see) sooner rather than later can only improve the chances of reducing your child’s X-ray exposure when managing scoliosis. In our scoliosis program, we attempt to reduce scoliosis rotation for postural improvement to help stop progression or improve scoliosis. Fortunately, we can effectively monitor scoliosis rotation between x-rays via Scoliometer™. This helps keep x-ray exposure to the absolute minimum.
(1) http://hps.org/documents/Medical_Exposures_Fact_Sheet.pdf
(2) Chamberlain CC, Huda W, Hojnowski LS, Perkins A, Scaramuzzino A. Radiation doses to patients undergoing scoliosis radiography. Br J Radiol. 2000 Aug; 73(872):847-53.
(3) Steven M. Presciutti, MD, Teja Karukanda, BS, Mark Lee, MD. Management decisions for adolescent idiopathic scoliosis significantly affect patient radiation exposure. The Spine Journal 14 (2014) 1984-1990.