The Cobb method of measuring scoliosis is the basis for diagnosis, prognosis and standard of care for treatment. Using the Cobb method, the Cobb angle (some refer to it as Cobb’s angle) is determined. This measurement is an important aspect of scoliosis to understand. Understanding Cobb’s method a little better may help you gain insight and help with the decision-making process for scoliosis treatment.
There’s a paper on scoliosis radiology that is worth a look. It may help you understand some of the nuances and limitations of the Cobb method. The review discusses how Cobb angle is determined and will hopefully take the mystery out of those degree* measurements the doctor provides you with.
About Cobb angle (according to citation below):
- Cobb angle is a two-dimensional representation of a three-dimensional condition.
- Cobb angle can be determined digitally or manually, both are reliable, but digitally is slightly more accurate.
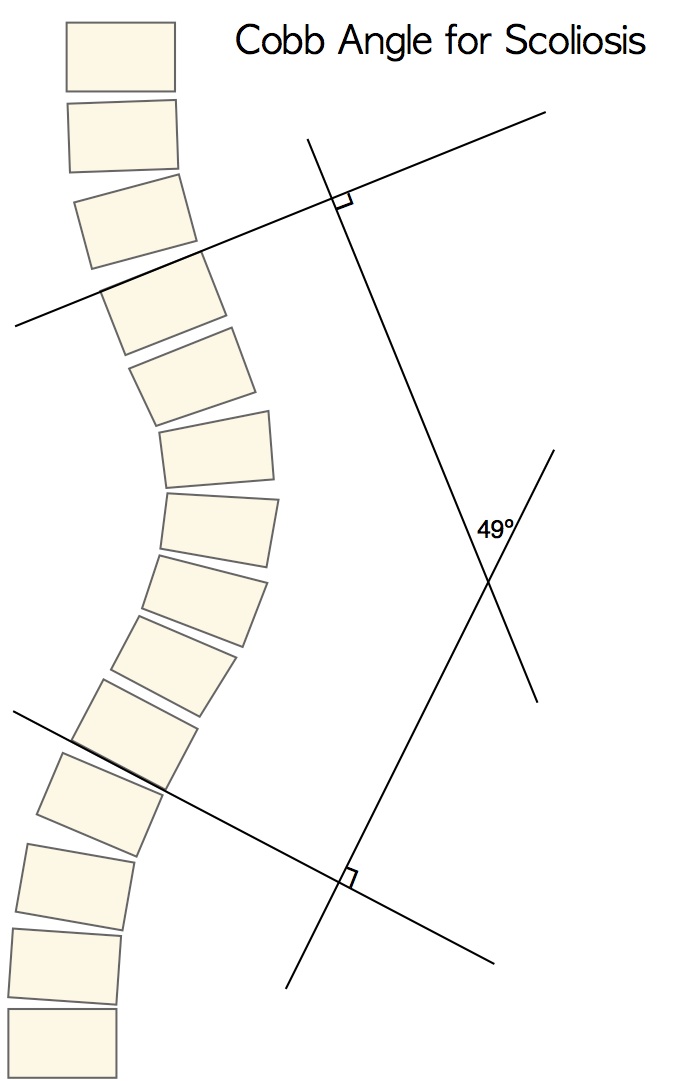
- “Cobb angle…is formed by the intersection of two lines, one parallel to the end plate of the superior [top] end vertebra and the other parallel to the end plate of the inferior [bottom] end vertebra.” When measuring practitioners should use the most tilted vertebrae.
- A 5º variation of Cobb angle may be observed over the course of the same day, worsening later in the day.
- Intra-observer variation of 5º to 10º can occur when measuring Cobb angle.
- Inter-observer variation can exceed intra-observer variation (i.e. one doctor’s measurements may be more than 10° different than another doctor’s measurements).
- A total error of a 2º to 7º variation can occur as a result of differences in acquisition methods.
- Because of vertebral rotation associated with scoliosis, the patient may stand slightly differently from one x-ray to the next, which can slightly skew the measurement.
Due to these variables, we encourage parents and patients not to fixate too much on the Cobb angle number. There are other factors that should be considered when it comes to scoliosis, such as postural appearance, angle of trunk rotation, spinal stabilization, and overall health and function are all part of the bigger picture.
While the Cobb method of measuring scoliosis is an important number for decision-making and making recommendations, we find that some parents tend to get hung up on the number (i.e. degree of scoliosis). This is understandable since parents are concerned but you should remember a change of just a couple of degrees is considered within the margin of error of measurement (5º) and not a huge cause for alarm.
When progression occurs and is greater than 5º, or a scoliosis continues to progress with each x-ray, parents and patients should take a proactive role in scoliosis management. Risser sign (stage of growth) should always be factored into the equation. It is only in rare instances that very mild curves will reduce spontaneously, and in scoliosis of 15º or more this almost never happens.
Our mission is to guide parents, their children, and adults with scoliosis through the process. Keep in mind that it is a lot easier to treat curves under 30º successfully–meaning the potential to achieve curve reduction. It is for this reason that we recommend parents of children with scoliosis take action sooner rather than later when possible.
* Cobb angle and scoliometer (measures vertebral rotation)–are different scoliosis measurements; however, both are measured in degrees, so it can be confusing. To read more on scoliosis measurements, link here.
Hana Kim, Hak Sun Kim, Eun Su Moon, Choon-Sik Yoon, Tae-Sub Chung, Ho-Taek Song, Jin-Suck Suh, Young Han Lee, Sungjun Kim. Scoliosis imaging: what radiologists should know. Radiographics. 2010 November; 30(7): 1823–1842.