What is progressive scoliosis?
Progressive scoliosis is a spinal curvature that increases more than 5º in Cobb angle within 6 months as measured on the AP/PA view of a full spine x-ray. There is no foolproof way for physicians to determine whether scoliosis will get worse after a diagnosis, predict whose scoliosis will be progressive and whose will stabilize, or to what degree. Estimating progression risk depends upon a combination of several factors.

Doctors may differ in their opinions of which factors may contribute to a progressive scoliosis. A 1984 study by Lonstein and Carlson used current age, Cobb angle, and Risser sign. However, each patient should be assessed individually and additional factors considered. At what age was scoliosis diagnosed? What was the child’s Cobb angle at the time of the diagnosis? Is there a family history of scoliosis? It is also necessary to consider the sagittal plane, vertebral rotation and its rate of increase, curve flexibility/rigidity, and gender – in girls: has menarche occurred, in boys: has voice change occurred? It is expected that girls with scoliosis who have not yet reached menarche will continue to grow and be at risk of progression; for the boys, it’s not unreasonable to think that growth can continue into the later teen years. In both these cases, it is important to be proactive to work to prevent scoliosis from becoming progressive and to improve or at least stabilize the curve through corrective bracing and scoliosis exercise rehabilitation. Curve-pattern and joint laxity may be other considerations. Joint laxity may be indicative of a connective tissue disorder. If your child shows an indication of joint laxity don’t be alarmed, just have it checked out for an accurate diagnosis.
The Vicious Cycle can Lead to a Progressive Scoliosis
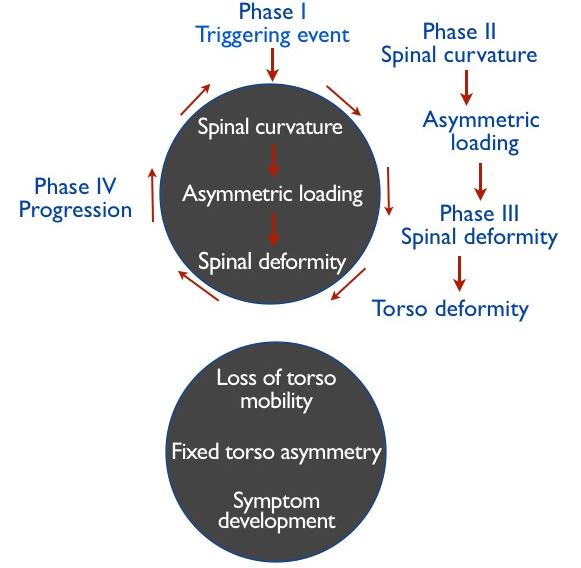
It is worth noting that regular activities and daily habits can have a potentially negative impact on scoliosis when the activity is performed repeatedly. This may potentially stimulate curve progression according to a theory known as the ‘vicious cycle’ of scoliosis progression. (Roaf 1960, Stokes 1996)
This following diagram of the vicious cycle theory illustrates how scoliosis may become progressive:
How do doctors predict whether scoliosis will become progressive?
No doctor knows for sure whether your child’s scoliosis will become progressive. Physicians will consider your child’s case individually, rely on their clinical experiences and some may use the Lonstein and Carlson (1984) equation (referenced below) to predict whether an adolescent’s curve will remain stable or get worse:
Progression Factor = Cobb Angle – (3 X Risser sign) / Chronological age
The ‘progression factor’ is then matched to a corresponding ‘nomogram’. Where a child’s ‘factor’ falls on the nomogram indicates their corresponding percentage risk of progression. There are several criticisms of this method of determining progression and the authors themselves state clearly that the lower end of the nomogram, indicating less risk of progression, is likely to be much more accurate than the upper end of the nomogram. There were far fewer subjects in the study with a higher degree of scoliosis at the upper end. Also, the study only included subjects with Cobb angles up to 29º.
Cobb angle is the measurement of scoliosis curve degree derived from an analysis of the vertebral positions of the spine on a full spine AP/PA x-ray view.
Risser is an estimate of growth potential based on a visual inspection of the amount of ossification of the iliac crest on x-ray. To determine Risser, doctors assign a grade on a scale of 0-5. A Risser of 0 indicates significant growth potential and a Risser of 5 indicates that a child is at skeletal maturity – no remaining growth. There is a small subset of patients we’ve seen who have experienced continued progression of a curvature despite being a Risser 4- 5. For this reason, we think it is best to err on the side of caution when discontinuing brace wear.
The progression factor equation does not take several of the other factors we mentioned earlier into account. This illustrates the individuality of scoliosis and the challenges of predicting progression. Certainly, if there is a family history (either parent, aunts or uncles, siblings, grandparents, etc.) parents must be highly vigilant and request that their pediatrician, chiropractor, physical therapist perform a simple scoliometer reading at regular check-ups as adolescence approaches.
An x-ray of the hand is sometimes taken to help determine ‘bone age.’ The purpose of this is to determine if biological age is in sync with the bone age indicated on the image. If bone age is more advanced, this helps doctors with their guesstimations about future growth.
Sometimes a family is vigilant and scoliosis seems to suddenly appear. Several parents and patients have reported discovering scoliosis accidentally after a chest x-ray for a respiratory illness. If there is a family history of scoliosis, visually check for scoliosis –frequently.
At Scoliosis 3DC® we teach patients how to interrupt the vicious cycle of scoliosis using our five-part Schroth method exercise program and corrective bracing if desired. If your goal is to help stabilize your or your child’s scoliosis through the most effective techniques possible, please give us a call to learn more about our scoliosis programs. We’re here to help!
References
Roaf, R. Vertebral growth and its mechanical control. Journal of Bone & Joint Surgery, 42-B: 40-59, 1960.
Stokes IAF, Spence H, Aronsson DD, Kilmer N: Mechanical modulation of vertebral body growth: implications for scoliosis progression. Spine, 21(10): 1162-1167, 1996.
Lonstein JE, Carlson JM. The prediction of curve progression in untreated idiopathic scoliosis during growth. J Bone Joint Surg Am. 66(7):1061–1071, 1984.